Want to Buy Tirzepatide Online? Here’s What You Need to Know First

If you’ve been researching peptides recently, there’s a good chance you’ve come across tirzepatide. Interest in tirzepatide has grown rapidly over the last few years, with researchers, scientists, and the general public all wanting to learn more about how this peptide works and why it has attracted so much attention. If you’re searching for information about tirzepatide peptides in the UK, this guide explains the basics, how it differs from other well-known peptides, and what to look for when sourcing research-grade materials. What Is Tirzepatide? Tirzepatide is a synthetic peptide that interacts with two naturally occurring signalling pathways within the body. Unlike earlier compounds that focus on a single pathway, tirzepatide is often described as a dual-action peptide because it interacts with both GIP and GLP-1 related receptors. This dual-pathway approach is one of the main reasons it has become such a widely discussed compound in recent years. Many researchers view tirzepatide as a significant development within the peptide field because of how it differs from previous generations of compounds. Why Is Tirzepatide So Popular? One reason tirzepatide has generated so much interest is the amount of research that has been conducted around it. Studies have explored its effects on appetite-related signalling, energy balance, and metabolic processes. As a result, it has become one of the most talked-about peptides currently available for research purposes. For those interested in learning more about how tirzepatide compares to other compounds, you may also find our guide on Semaglutide vs Tirzepatide helpful. Tirzepatide vs Semaglutide A common question people ask is how tirzepatide differs from semaglutide. While both compounds are frequently discussed in similar conversations, there are some important differences. Semaglutide Single-pathway interaction Well-established peptide Often described as steady and predictable Tirzepatide Dual-pathway interaction More recent development Often described as a next-generation peptide You can read a more detailed breakdown in our Semaglutide vs Tirzepatide Comparison Guide. What Should You Look for When Buying Tirzepatide Peptides in the UK? Not all suppliers are the same. When evaluating a supplier, it’s worth considering: Quality Control Look for suppliers that clearly explain their quality standards and provide transparency around their products. Consistency Research relies on consistency and reproducibility, so reliable sourcing is important. Clear Product Information A reputable supplier should provide clear information about the product, storage requirements, and intended research use. Research-Only Positioning Products should be clearly labelled and supplied for research purposes only. Why Do Tirzepatide Products Say “Not for Human Consumption”? This is another question that comes up regularly. Research peptides are often labelled as: Research Use Only Not for Human Consumption Not Intended for Human Use These statements exist to clearly define how the products are classified and supplied. If you’re interested in understanding this in more detail, read our article: What Does Not for Human Consumption Actually Mean? The Growing Interest in Next-Generation Peptides Tirzepatide helped bring increased attention to dual-action peptides, but the peptide landscape continues to evolve. Newer compounds such as retatrutide are now attracting significant interest because of their broader signalling profiles and ongoing research. For readers interested in emerging developments, our guide on Why Retatrutide Is Getting So Much Attention explores this topic further. Finding Research-Grade Tirzepatide in the UK When sourcing tirzepatide online in the UK, it’s important to focus on transparency, consistency, and quality. Reliable suppliers such as TrimFast will provide clear information about their products, maintain high standards, and ensure materials are supplied within an appropriate research framework. For researchers looking to explore available options, you can browse our current range of Tirzepatide Products here. Final Thoughts Tirzepatide has become one of the most widely discussed peptides in recent years, and it’s easy to see why. Its dual-pathway design, growing body of research, and increasing visibility have helped make it a major topic of interest within the peptide community. Whether you’re new to peptides or simply looking to expand your understanding, taking the time to learn about compounds like tirzepatide can help provide valuable context for the wider research landscape. Related Articles [Semaglutide vs Tirzepatide: What’s the Difference?] [How Does Tirzepatide Work?] [What Does Research Use Only Mean?] [Why Is Retatrutide Getting So Much Attention?] [Browse Tirzepatide Products]
Not for Human Consumption: What Does It Actually Mean?

If you’ve been looking into peptides or similar compounds, you’ve probably seen phrases like “not for human consumption” or “for research use only.” Even here at TrimFast , we categorize and label our own products like this. At first glance, it can sound confusing — or even concerning. So what does it actually mean? The simple explanation The terms “Not for human consumption” and “research use only” mean the product has not been approved to be used as a medicine by pharmaceutical bodies such as the FDA. Instead, it’s supplied for things like: Laboratory research Scientific study Analytical testing That’s it. It’s about intended use and classification, not necessarily anything else. As of 2026 , there are only a couple of branded versions of the compounds that have been given approval to be marketed as a medicine, and these are typically prescribed versions of the compound in prepared injectable states, rather than the freeze dried, raw compounds sold buy vendors such as Trimfast What it DOES mean When you see “not for human consumption” and “research use only” it means: The product is supplied for research purposes and not intended for human use It is not licensed as a medicine so cannot be sold as such The supplier is operating within a research-use framework, such as for academic use What it DOESN’T mean This is where a lot of confusion comes in. It does NOT automatically mean: The product is toxic or dangerous. The compound is ineffective or low quality The supplier is doing something wrong or illegal It simply means the product is not positioned or approved as a medical treatment. Why these labels exist For a substance to be approved for human use, it has to go through a long process: Clinical trials and safety testing Regulatory approval with strict manufacturing standards Medical Licencing Many compounds in the peptide space are still being studied or explored, so they don’t go through that full approval process. Because of that, they must be clearly labelled to reflect their research-only status. However, For GLP-1’s like tirzepatide and semaglutide, while these have been trialed, tested and even approved for human use, they are currently only allowed to be marketed as medicine by licenced pharmaceuticals, such as Elililly with Mounjaro and Novonordisk with Wegovy. For peptide suppliers such as trimfast, we must adhere to the compliancy rules and only market as research only use. Why you see it so often In this space, these labels are standard. Many compounds are: Still being studied Widely discussed Not yet approved as medicines So suppliers use clear wording to make sure there’s no confusion about how the products are intended to be used. The key distinction There’s an important difference between: Approved medicines (regulated for human use) Research compounds (used for study and investigation) The “not for human consumption” label exists to clearly separate those two categories. Why this matters Understanding this helps set the right expectations. It ensures: Transparency from suppliers Clear positioning of products Better understanding for customers The bottom line “Not for human consumption” isn’t a warning that something is bad — it’s a clarification of how the product is classified. It simply means the product is intended for research use and has not been approved as a medicine. Learn more about our research use peptides here
Semaglutide vs Tirzepatide: Which Is Better for Appetite and Cravings?
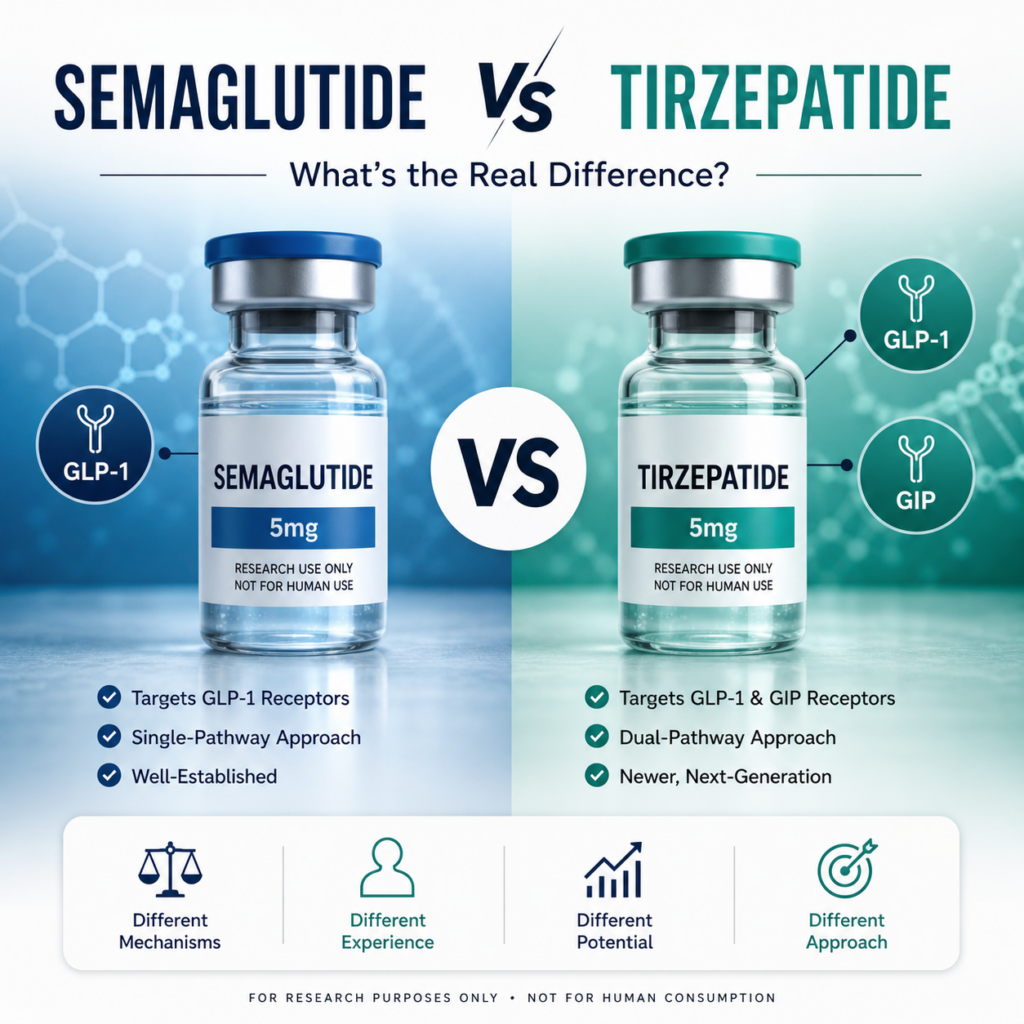
If you’ve been looking into options related to weight management, you’ve likely come across semaglutide and tirzepatide. Both are often discussed in relation to appetite, food intake, and cravings — but they don’t work in exactly the same way. So what’s the real difference when it comes to how they’re described in everyday terms? 🧠 How They Affect Appetite Both compounds are commonly associated with how the body regulates hunger signals. Semaglutide is often described as helping to: Reduce overall appetite Increase feelings of fullness Slow down how quickly hunger returns after eating Tirzepatide, on the other hand, is often talked about as having a broader effect due to how it interacts with more than one signalling pathway. Stronger appetite suppression (as often described) Longer-lasting fullness Reduced interest in food in general 🍽️ Cravings and Food Focus One of the biggest differences people talk about is how these compounds may influence cravings. With semaglutide, discussions often focus on: Reduced portion sizes Less frequent snacking Better control over eating habits With tirzepatide, the conversation often goes a step further: Less “food noise” (constant thinking about food) Lower interest in high-calorie foods A more noticeable shift in eating behaviour ⚖️ Intensity: Mild vs Stronger Approach In simple terms, the difference is often described like this: Semaglutide → steady, gradual, more predictable Tirzepatide → stronger, more noticeable effects This doesn’t mean one is better — it just reflects how people typically describe their differences. 📊 Why Tirzepatide Gets More Attention Tirzepatide is often seen as a “next step” because of its dual-action design. In everyday terms, that means it may influence more of the body’s appetite-related signals at once — which is why it’s often talked about as more powerful. 💬 Which One Is Right? This comes down to what someone is looking for: A more gradual and steady approach → semaglutide is often discussed A stronger, more noticeable shift in appetite → tirzepatide is often highlighted Both sit in the same category, but they’re typically positioned at slightly different levels. 🧩 The Bottom Line Semaglutide and tirzepatide are often compared because they both relate to appetite and weight management discussions — but they’re not identical. Semaglutide is usually seen as a more established and steady option, while tirzepatide is often described as a more advanced and intensive alternative. The key difference comes down to how strongly they are perceived to influence appetite, cravings, and overall eating behaviour. 🔗 Related Reading Semaglutide vs Tirzepatide (Research Breakdown) How Does Tirzepatide Work? View Tirzepatide Products View Semaglutide Products
Semaglutide vs Tirzepatide vs Retatrutide: A Complete Guide to Weight Loss Peptides
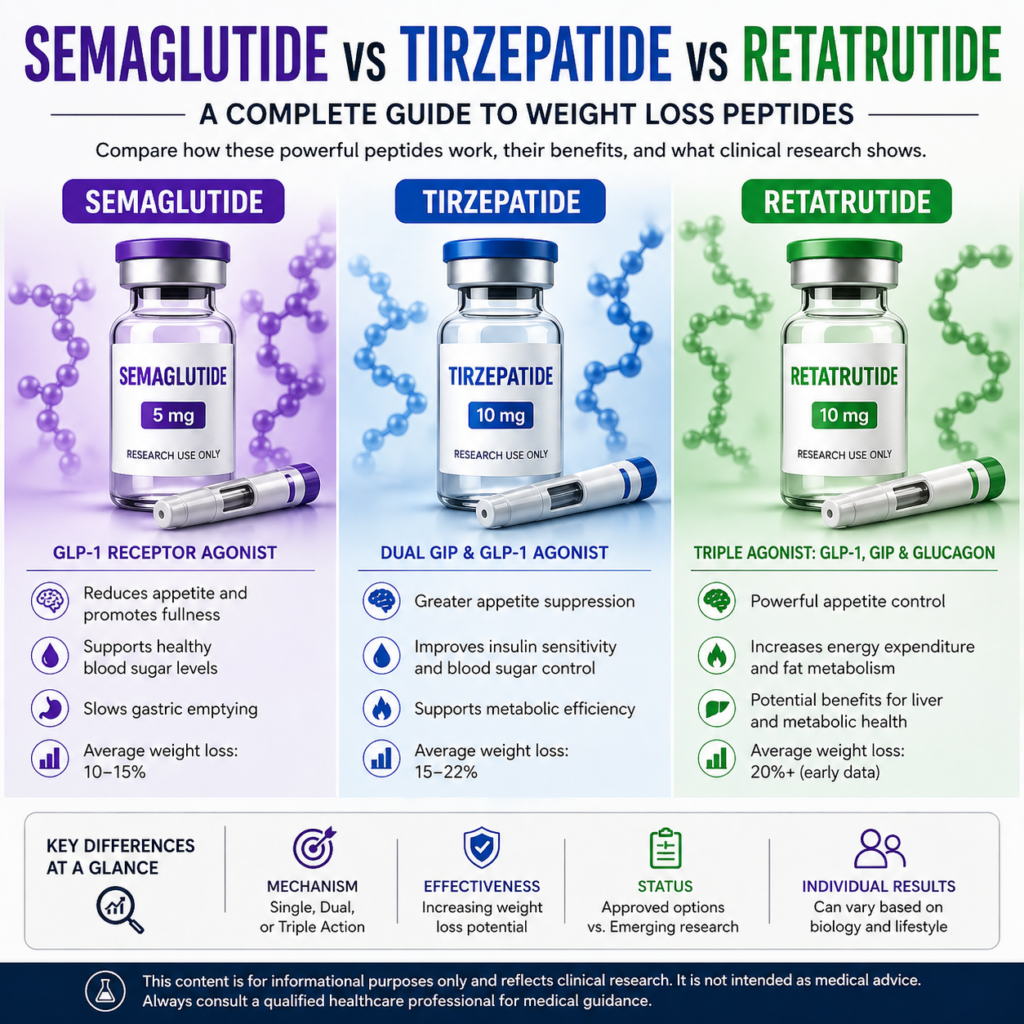
If you’ve been researching weight loss peptides or GLP-1 medications, you’ve likely come across three names: semaglutide, tirzepatide, and retatrutide. These compounds are part of a new wave of incretin-based therapies that are changing how weight management and metabolic health are approached in clinical settings. But while they’re often grouped together, they work differently—and their results can vary significantly. What Are GLP-1 and Incretin-Based Therapies? GLP-1 (glucagon-like peptide-1) is a hormone involved in: Appetite regulation Blood sugar control Slowing digestion Energy balance Modern peptide therapies are designed to mimic or enhance these natural processes. 👉 Related: Explore Semaglutide 👉 Related: Explore Tirzepatide Semaglutide: The Foundation of Modern GLP-1 Weight Loss Semaglutide is one of the most widely used GLP-1-based therapies. How semaglutide works It mimics the GLP-1 hormone, leading to: Reduced appetite Slower gastric emptying Improved blood glucose regulation Clinical performance Studies have shown: Around 10–15% average weight loss Consistent appetite reduction over time Additional benefits Improved metabolic markers Cardiovascular risk reduction in certain populations Summary Semaglutide is often considered: Well-established Predictable A strong starting point in GLP-1 therapy Tirzepatide: Dual-Hormone Metabolic Enhancement Tirzepatide builds on GLP-1 by targeting an additional pathway. How tirzepatide works It activates: GLP-1 receptors GIP receptors (enhancing insulin sensitivity and metabolic response) Clinical performance Trials have reported: 15–22% weight loss depending on dose Strong improvements in insulin regulation Additional benefits Greater appetite suppression for many individuals Enhanced metabolic efficiency Summary Tirzepatide is often described as: More potent than semaglutide Faster in producing noticeable results 👉 Learn more: View Tirzepatide options Retatrutide: The Next-Generation Triple Agonist Retatrutide represents a newer class of triple agonist peptides. How retatrutide works It targets: GLP-1 GIP Glucagon receptors The glucagon component may: Increase energy expenditure Promote fat oxidation Clinical performance (early data) Weight loss exceeding 20% in some trial groups Effects appear strongly dose-dependent Additional areas under research Liver fat reduction Metabolic rate changes Long-term energy balance Summary Retatrutide is: Highly promising Mechanistically advanced Still under investigation 👉 Explore further: Learn more about Retatrutide Key Differences Between Semaglutide, Tirzepatide, and Retatrutide Feature Semaglutide Tirzepatide Retatrutide Mechanism GLP-1 GLP-1 + GIP GLP-1 + GIP + Glucagon Weight Loss ~10–15% ~15–22% 20%+ (early data) Status Approved Approved Investigational Complexity Moderate Higher Advanced Which Peptide Performs Best? The answer depends on what you’re measuring. Appetite control: strong across all three Metabolic impact: increases from semaglutide → tirzepatide → retatrutide Weight loss potential: highest in newer multi-agonist compounds However: Individual response varies Tolerability plays a major role Dose escalation affects outcomes significantly What Real-World Use Looks Like In clinical practice and research settings: Effects build over weeks to months Results improve with consistent use Lifestyle factors still play an important role These are not instant solutions—but rather tools that influence long-term metabolic regulation. A Smarter Way to Compare These Peptides Instead of asking “which is best,” it’s often more useful to think in terms of progression: Semaglutide → established GLP-1 baseline Tirzepatide → enhanced dual-pathway approach Retatrutide → next-generation metabolic targeting 👉 Browse all compounds: View research peptide catalogue Final Thoughts Semaglutide, tirzepatide, and retatrutide represent a clear evolution in metabolic therapies. Each step introduces: more complex mechanisms stronger potential effects and new considerations around tolerability and long-term use As research continues, these compounds are shaping the future of weight loss treatments and metabolic health strategies. Continue Exploring If you’re looking to go deeper: Semaglutide overview Tirzepatide details Retatrutide research This content is for informational purposes only and based on published clinical research. It is not intended as medical advice.
The Oral Tirzepatide Pill: Will It Be as Effective as the Injection?
In the last few years, medications like tirzepatide have drawn huge attention for their role in weight management and metabolic health. At the moment, tirzepatide is available only as a weekly injection, but pharmaceutical companies are actively working on tablet versions of similar drugs — and the idea of a pill instead of a needle has understandably caught a lot of interest. So the question many people are asking is simple: if a tirzepatide pill eventually becomes available, will it work as well as the injectable version? Let’s look at what the latest research and developments suggest. Why an Oral Version Is Being Developed The main reason companies are exploring oral versions of these medications is convenience. Many people dislike injections, even if they’re only once a week. A tablet taken daily could make treatment easier for some people and potentially increase access worldwide. Pharmaceutical companies have already had success with oral versions of related medications. For example, an oral form of semaglutide, Rybelsus, was approved for diabetes several years ago, showing that the hormone-based mechanism can be delivered in pill form. But developing an effective pill isn’t as straightforward as it sounds. Why Pills Are Harder to Develop The biggest challenge is absorption. When a medication is injected, it enters the bloodstream directly. But when a pill is swallowed, it has to survive stomach acid, digestive enzymes, and the intestinal barrier before it can be absorbed. Because of this, oral versions of hormone-based medications often require higher doses or special delivery technology to achieve the same biological effect. That’s why many experts expect injectable forms to remain the most reliable and consistent delivery method, at least for now. How Effective Could a Pill Be? Early research on oral GLP-1–style medications suggests they can still produce meaningful results, but often not quite at the same level as injections. For example, recent trials of new oral metabolic drugs have shown weight reductions of roughly 12–14% of body weight, while some injectable therapies can reach 15–20% or more in clinical studies. That doesn’t mean pills won’t work — just that the injectable versions currently set a very high benchmark. Injectable tirzepatide in particular has produced some of the strongest outcomes in its class, which makes it harder for a tablet version to match those results exactly. Will There Be an Oral Tirzepatide Soon? At the moment, no oral tirzepatide product has been officially approved, and the injectable form remains the only clinically validated version. However, pharmaceutical companies are investing heavily in oral metabolic treatments. Several pill-based drugs targeting the same appetite-related pathways are currently in late-stage clinical trials, and regulatory submissions are expected within the next few years. In other words, while a true tirzepatide tablet isn’t available yet, the shift toward oral metabolic therapies is clearly underway. The Bottom Line An oral version of tirzepatide — or a similar medication — would likely be welcomed by many people simply because it removes the need for injections. However, based on current research, injections may still provide more consistent and powerful results, mainly because the medication reaches the bloodstream more directly. That said, pill-based therapies are improving quickly. In the coming years, the difference between injections and tablets may become much smaller as new delivery technologies evolve. For now, the injectable form remains the most established and studied option, while oral versions represent the next stage of development in metabolic medicine. Potential Side Effects Being Studied in Current Trials As with most medications that affect appetite and metabolism, researchers closely monitor potential side effects when studying GLP-1–related treatments and similar compounds. The most commonly discussed effects in clinical trials tend to involve the digestive system. Participants in studies sometimes report symptoms such as nausea, reduced appetite, stomach discomfort, or mild gastrointestinal changes, particularly during the early stages of treatment. These effects are often described as temporary and may lessen as the body adjusts over time. Researchers also pay attention to factors like dosage, frequency, and how the medication is delivered, as these can influence how the body responds. For example, a daily pill may interact differently with digestion compared to a weekly injection, which is one reason scientists are carefully studying oral versions before any approvals. As research continues, long-term safety data will play a key role in determining how oral metabolic treatments compare with existing injectable options. Why GLP-1 Pills Could Be the Next Big Shift The biggest appeal of pill-based metabolic medications is simple: ease of use. For many people, taking a daily tablet feels more familiar and convenient than using a weekly injection. This could potentially lower the barrier for people who are uncomfortable with needles or who prefer a more traditional medication routine. There are also practical benefits from a healthcare perspective. Tablets can be easier to transport, store, and distribute, which may improve accessibility in some healthcare systems. However, convenience isn’t the only factor researchers are considering. Scientists are also exploring whether new oral delivery technologies can improve how these medications are absorbed in the body. If future pills can achieve similar consistency and effectiveness to injections, they could represent a significant shift in how metabolic treatments are used. For now, injections remain the most established option, while oral alternatives represent an exciting area of ongoing development.
Weight Loss, Peptides, and Metabolic Research: What the Science Says

Weight loss remains one of the most searched health topics in the UK. As conversations around obesity, metabolic health, and appetite regulation grow, many people are encountering terms such as peptides, GLP-1, semaglutide, and tirzepatide — often without clear explanations. This article provides an easy-to-understand overview of how weight regulation works, why peptides are being studied in scientific research, and what current evidence does (and does not) show. All information is presented for educational purposes only and reflects published research, not treatment advice. Why Weight Loss Is More Complex Than Diet and Exercise Alone While lifestyle choices are important, body weight is influenced by a combination of biological systems, including: Hormone signalling between the gut and brain Appetite regulation and satiety cues Blood glucose control Metabolic rate and energy balance Scientific research increasingly shows that weight management is not purely behavioural. Hormonal signalling pathways play a central role in how hunger, fullness, and energy storage are regulated. This is one reason peptides involved in metabolic signalling are being widely studied in clinical and laboratory settings. What Are Peptides? Peptides are short chains of amino acids that act as biological messengers. Many naturally occurring hormones are peptides, involved in digestion, insulin signalling, and appetite regulation. In research contexts, synthetic peptides are designed to interact with specific receptors to better understand how metabolic pathways function. These compounds are studied under controlled conditions to explore their effects on glucose metabolism, appetite signalling, and energy regulation. Two peptides frequently referenced in UK and international research literature are: Semaglutide – a GLP-1 receptor agonist Tirzepatide – a dual GIP and GLP-1 receptor agonist Why Peptides Are Studied in Weight Management Research From a scientific perspective, peptides are of interest because they interact with pathways related to: Appetite signalling and satiety Post-meal glucose regulation Hormone-mediated metabolic responses Gastrointestinal signalling processes Rather than acting as traditional appetite suppressants, these compounds are studied for how they influence existing physiological systems already present in the body. This distinction is important when interpreting media coverage or online discussions around peptide research. The Science Behind GLP-1 and GIP Pathways Understanding GLP-1 and GIP in Simple Terms GLP-1 (glucagon-like peptide-1) and GIP (glucose-dependent insulinotropic polypeptide) are hormones released after food intake. In research environments, these pathways are examined for their role in: Communicating fullness to the brain Regulating insulin secretion Influencing glucose response after meals Semaglutide is designed to interact with GLP-1 receptors, while tirzepatide interacts with both GLP-1 and GIP receptors. Researchers study how these interactions affect metabolic signalling in controlled studies. What Current Research Can and Cannot Confirm Although peer-reviewed studies have produced extensive data, there are important limitations to consider: Many studies are conducted under tightly controlled clinical conditions Individual responses vary significantly Long-term population-level data continues to develop Results from studies do not guarantee outcomes for individuals For these reasons, responsible scientific discussion avoids definitive claims and focuses on mechanisms, observations, and ongoing research. Growing UK Interest in Peptide Research In the UK, public interest in peptides has increased alongside wider discussions around: Obesity and metabolic health NHS prescribing capacity Advances in endocrinology research New approaches to appetite and glucose regulation Search trends show rising UK queries for phrases such as “GLP-1 research,” “semaglutide studies,” and “metabolic peptides”, reflecting curiosity about the science rather than clinical guidance. Regulatory Context in the UK In the UK, compounds such as semaglutide and tirzepatide are classified as prescription-only medicines when used clinically. Any non-clinical discussion must remain informational, non-promotional, and aligned with regulatory guidance. Scientific references relate to published research and approved clinical data, not personal use or treatment recommendations. Key Takeaway Peptides such as semaglutide and tirzepatide are widely studied because of their role in metabolic and appetite-related signalling pathways. While research continues to expand, understanding the science, limitations, and regulatory framework is essential. Clear, evidence-based information helps separate genuine research from misinformation and exaggerated claims. Regulatory & Information Disclaimer This content is provided for educational and informational purposes only. It does not constitute medical advice, diagnosis, or treatment. References to peptides and metabolic research are based on publicly available scientific literature and regulated clinical data. Always consult a qualified healthcare professional for medical decisions.
Retatrutide: The Triple-Agonist Peptide Under Investigation — What We Know and What It Could Mean
Retatrutide is an investigational peptide being developed by Eli Lilly that has attracted attention in scientific and research communities for its potential effects on metabolic pathways related to overweight and obesity. Unlike currently approved medications such as semaglutide and tirzepatide, retatrutide acts on three hormone receptors — GLP-1, GIP, and glucagon — and is being studied in ongoing clinical trials. What Retatrutide Is (Mechanism of Action) Retatrutide is a triple-agonist peptide designed to activate three distinct receptors involved in glucose regulation, energy balance, and appetite: GLP-1 (glucagon-like peptide-1) — influences satiety and insulin secretion GIP (glucose-dependent insulinotropic polypeptide) — affects insulin and fat metabolism Glucagon receptor — may increase energy expenditure and influence fat usage This combination is distinct from: Semaglutide, which targets just GLP-1 Tirzepatide, which targets GLP-1 and GIP By engaging all three pathways, researchers hope retatrutide can produce broader metabolic effects than earlier agents, though much of this remains under investigation. Clinical Trial Results So Far Phase 2 and initial Phase 3 data suggest retatrutide may lead to marked reductions in body weight in adults with overweight or obesity: In Phase 2 studies, participants achieved dose-dependent weight reductions, with the highest doses showing mean reductions of around 24% after 48 weeks compared with placebo. Early Phase 3 topline results from the TRIUMPH-4 trial reported average weight decreases of approximately 28.7% at a 12 mg weekly dose among participants with obesity and related conditions. These figures, while promising in a research context, are preliminary and have not yet been confirmed in full, peer-reviewed publications. FDA Approval Status and Timeline As of early 2026: Retatrutide is not FDA-approved for weight management or any clinical use. The molecule remains under evaluation in multiple Phase 3 clinical trials (the TRIUMPH program). Regulatory filings (New Drug Application) and review timelines depend on the completion of these trials and subsequent regulatory assessments. Projections suggest a submission could occur in late 2026 or early 2027, with a standard review period potentially concluding in late 2027 to early 2028, although this could shift depending on data outcomes and regulatory decisions. Because retatrutide has not been approved by regulatory authorities, it is not legally available for clinical use or sale outside of research settings. Any products marketed as retatrutide outside of formal trials may be unsafe, unverified, and not compliant with regulatory standards. Comparing Retatrutide, Tirzepatide, and Semaglutide Retatrutide’s triple-agonist mechanism represents a conceptual advance over earlier agents: Semaglutide is a single-receptor GLP-1 agonist with a long track record of clinical research and regulatory approval. Tirzepatide is a dual GLP-1/GIP agonist, already approved and widely studied in large Phase 3 programs. Retatrutide, by adding glucagon receptor activation, has shown enhanced weight loss in early research settings, though head-to-head trials with approved medications are limited and safety profiles remain under definition. Some study syntheses suggest that triple-agonist approaches may yield greater average reductions in weight metrics than single or dual agonists in controlled settings, but differences in trial design and endpoints make careful interpretation essential. Safety and Evidence Limitations Because retatrutide is still investigational, its long-term safety profile is unknown. Early reports from trials note gastrointestinal effects such as nausea, diarrhea, and vomiting, similar to other incretin-modulating peptides. No comprehensive safety data from large, diverse populations are available yet, and rare or serious adverse events remain to be fully characterised. Continued monitoring and regulatory review will be needed as more Phase 3 data emerge. Could Retatrutide “Dethrone” Current Agents? Retatrutide’s early data suggest higher average weight reductions in research contexts than those reported with semaglutide or tirzepatide. However: Approved medications have robust safety and efficacy evidence from large Phase 3 trials and real-world experience. Retatrutide’s comparative performance relies on preliminary data and indirect comparisons, not direct regulatory-grade head-to-head trials. Whether it could become the dominant option will depend on final trial results, regulatory review, cost, prescribing practices, and long-term safety outcomes. Conclusion Retatrutide represents an innovative triple-agonist peptide under active investigation for metabolic effects in overweight and obesity. Early research shows promising reductions in body weight, and clinical trial timelines suggest regulatory decisions may unfold in late 2027 or later. Until regulatory approval is obtained, however, it remains an investigational compound, and any discussion of its use should be grounded in peer-reviewed research and regulatory status.
Semaglutide Tablets vs Injectable Semaglutide: A Research-Focused Comparison

Semaglutide is a glucagon-like peptide-1 (GLP-1) receptor agonist that has been widely studied in relation to glucose regulation and appetite-related biological pathways. While it is most commonly associated with injectable formulations, an oral (tablet) version has also been developed and approved for specific clinical indications. Although both formats contain the same active compound, the method of delivery introduces important scientific and pharmacokinetic differences. This article explores how oral and injectable semaglutide compare from a formulation and research perspective, rather than from a treatment or consumer standpoint. 1. Formulation and Delivery Method Injectable Semaglutide Injectable semaglutide is administered subcutaneously, allowing the peptide to enter systemic circulation without passing through the digestive system. This route avoids gastrointestinal degradation and is associated with relatively predictable absorption patterns. From a research perspective, injectable formulations are often used when: Controlled and consistent systemic exposure is required Long-acting pharmacokinetics are being examined Dose–response relationships need precise modelling Oral (Tablet) Semaglutide Oral semaglutide presents a distinct formulation challenge, as peptide compounds are typically broken down by stomach acid and digestive enzymes. To address this, oral formulations are developed alongside absorption-enhancing technologies designed to support uptake through the gastrointestinal lining. This makes oral semaglutide a useful case study in areas such as: Peptide stabilisation strategies Gastrointestinal absorption mechanisms Oral delivery of large-molecule compounds 2. Bioavailability and Absorption One of the most notable scientific differences between oral and injectable semaglutide lies in bioavailability. Injectable semaglutide is associated with higher and more predictable systemic exposure. Oral semaglutide has lower absolute bioavailability, with absorption influenced by factors such as timing of administration, stomach contents, and individual gastrointestinal physiology. These differences are of particular interest in pharmacokinetic research, especially when examining: Peak plasma concentrations Time to steady state Inter-individual variability 3. Dosing Considerations in Research Contexts Due to differences in absorption efficiency: Oral formulations are typically studied at higher nominal doses to achieve comparable systemic exposure. Injectable formulations allow for lower administered doses with more consistent plasma levels. For researchers, this distinction is relevant when designing studies involving: Dose scaling Exposure–response modelling Comparative pharmacology 4. Stability and Handling Considerations Injectable semaglutide is commonly supplied as a solution or as a reconstituted formulation, requiring controlled storage and handling conditions. Oral semaglutide, by contrast, must maintain: Solid-state stability Protection from moisture and heat Formulation integrity over time These differences make each format relevant for different areas of formulation science and stability research. 5. Why This Comparison Matters Although oral and injectable semaglutide involve the same active molecule, they are not interchangeable from a scientific or formulation standpoint. Each approach offers insight into different challenges within peptide drug development, including: Delivery system design Absorption enhancement Long-acting versus daily exposure models Understanding these distinctions is important when interpreting study outcomes or comparing data across trials that use different formulations. Summary Oral and injectable semaglutide represent two distinct strategies for delivering the same peptide compound. Injectable formulations are associated with predictable systemic exposure, while oral formulations highlight advances in peptide delivery and absorption technology. From a research and development perspective, both formats contribute valuable insights into GLP-1–based compounds and the broader field of peptide therapeutics. Limitations of Current Evidence While both oral and injectable semaglutide have been widely studied, several limitations in the current evidence base should be acknowledged. Direct head-to-head comparisons between the two formulations remain limited, with many studies evaluating each format separately under differing protocols, populations, and dosing schedules. This makes direct comparison more complex. Absorption variability, particularly with oral formulations, introduces additional uncertainty, as factors such as food intake, gastric emptying, and individual physiology can influence systemic exposure. Much of the existing data also focuses on short- to medium-term outcomes, with fewer long-duration studies examining extended exposure, long-term formulation stability, or comparative pharmacodynamics over time. As peptide delivery technologies continue to evolve, conclusions drawn from current formulations may require reassessment as new data emerges. Regulatory & Use Notice This content is provided for informational and scientific discussion purposes only. Semaglutide is a prescription-only medicine. No product, formulation, or route of administration is being promoted or recommended. References to dosing, delivery methods, or mechanisms relate to published research and regulatory-approved data and do not constitute medical advice.
Weight Change Following Discontinuation of Tirzepatide: A Review of Current Evidence
Background Recent public discussion has highlighted concerns regarding weight regain following discontinuation of GLP-1–based therapies such as tirzepatide. Media coverage referencing clinical trial data has suggested that cessation of treatment may be associated with reversal of weight-related and metabolic changes. This article reviews the current scientific literature to contextualise these findings and explore factors that may influence outcomes after treatment discontinuation. Evidence From Clinical Research GLP-1 receptor agonists, including semaglutide and the dual GIP/GLP-1 agonist tirzepatide, have been extensively studied in controlled clinical trial settings. Published trials have consistently demonstrated significant reductions in body weight over extended treatment periods when combined with structured lifestyle interventions. Reported outcomes from major studies indicate: Semaglutide has been associated with average reductions in body weight of approximately 10–15% over 12 months in trial populations. Tirzepatide has demonstrated higher average reductions in body weight in some studies over longer durations. These findings reflect outcomes observed under structured trial conditions and do not necessarily predict individual responses outside controlled environments. Observations Following Treatment Discontinuation Data from continuation and withdrawal phases of clinical trials, including studies such as SURMOUNT-4, indicate that participants who discontinued tirzepatide experienced partial weight regain over time. Associated changes were also observed in anthropometric and metabolic markers previously improved during active treatment. Importantly, these findings reflect a return toward baseline physiological and behavioural patterns rather than evidence of adverse biological effects caused by discontinuation itself. Mechanistic Considerations GLP-1–based compounds influence appetite regulation, gastric emptying, and energy intake through central and peripheral pathways. During active treatment, these mechanisms may facilitate reduced caloric intake without conscious restriction. Upon discontinuation, appetite signalling and food-related cues may gradually return toward pre-treatment levels. In the absence of sustained dietary or behavioural adjustments, increased energy intake may occur, contributing to gradual weight regain. This phenomenon aligns with established principles of energy balance rather than treatment-specific pathology. Role of Behavioural and Lifestyle Factors Clinical trial protocols typically include structured dietary guidance, monitoring, and behavioural support. Outside of these settings, individuals discontinuing treatment may not receive comparable support, which may influence post-treatment outcomes. Current evidence suggests that weight trajectory following discontinuation is influenced by multiple factors, including: Dietary patterns Physical activity levels Behavioural habits established during treatment Access to ongoing professional support Interpretation of Findings Weight regain following discontinuation of pharmacological weight-management interventions is not unique to GLP-1–based compounds and has been observed across multiple therapeutic classes. The available data do not suggest irreversible metabolic changes or treatment-induced dependency, but rather reflect the absence of ongoing pharmacological appetite modulation. Limitations of Current Evidence While the existing body of research provides valuable insights into weight change following discontinuation of GLP-1–based therapies, several limitations should be acknowledged. Many findings are derived from controlled clinical trial environments, where participants receive structured dietary guidance, monitoring, and follow-up that may not reflect real-world conditions. Outcomes observed in these settings may therefore differ from those seen in broader, more heterogeneous populations. In addition, discontinuation phases within trials are often limited in duration, meaning long-term trajectories beyond the study period remain incompletely characterised. Individual variability in behavioural adaptation, lifestyle factors, and metabolic response further complicates interpretation of aggregate results. Finally, much of the available data focuses on population-level trends rather than individual outcomes. As such, conclusions regarding post-treatment weight change should be interpreted as observational rather than predictive, and ongoing research is required to better understand long-term patterns across diverse study populations. Conclusion The existing body of research indicates that discontinuation of tirzepatide may be associated with partial weight regain in some individuals, particularly in the absence of sustained lifestyle adaptations. These findings underscore the importance of contextualising clinical trial data and avoiding oversimplified interpretations of post-treatment outcomes. Ongoing research continues to explore long-term management strategies, behavioural interventions, and the durability of treatment-associated changes following cessation of GLP-1–based therapies.
Tirzepatide vs Semaglutide: A Research-Based Comparison and Evolving Treatment Approaches

In recent years, clinical interest in GLP-1–based therapies has increased significantly. Among the most frequently discussed compounds are semaglutide and tirzepatide, both of which are studied for their roles in metabolic health and weight-management research. Although these medications are often mentioned together, they differ in how they interact with metabolic pathways. Understanding those differences — and how treatment approaches may evolve over time — can help place current research into context. This article provides an informational overview only, drawing on published research and educational resources. It does not offer medical advice or recommendations. Decisions about treatment should always be made in consultation with a qualified healthcare professional. Overview of Semaglutide Semaglutide belongs to a class of medications known as GLP-1 (glucagon-like peptide-1) receptor agonists. It was initially developed for glycaemic control in type 2 diabetes and has since been widely studied in the context of metabolic and weight-related research. How Semaglutide Is Understood to Function Based on current evidence, semaglutide is associated with effects such as: Modulation of appetite-related signalling Increased feelings of fullness after eating Slower gastric emptying Support for more stable blood glucose regulation In clinical settings, semaglutide is often introduced using a gradual dose-escalation approach, allowing physiological adaptation over time. Because of this structured introduction, it is frequently discussed in research as a foundational GLP-1-based option. Overview of Tirzepatide Tirzepatide is described in the literature as a dual-agonist peptide, as it interacts with two hormone receptors involved in metabolic regulation. Unlike semaglutide, which targets GLP-1 receptors alone, tirzepatide acts on: GLP-1 receptors GIP (glucose-dependent insulinotropic polypeptide) receptors Why Dual-Pathway Activity Is Studied By engaging two incretin pathways, tirzepatide is being researched for its potential to: Influence appetite and satiety through multiple mechanisms Support glycaemic regulation via complementary hormonal effects Produce distinct metabolic responses compared with single-pathway agents Because of this dual activity, tirzepatide is often examined in studies involving individuals who have already been exposed to GLP-1–based therapies. Semaglutide and Tirzepatide: Key Research Differences While both compounds fall under the broader incretin-based category, research highlights several distinctions. Mechanism of Action Semaglutide: GLP-1 receptor agonist Tirzepatide: Dual GIP and GLP-1 receptor agonist Appetite and Satiety Signalling Both compounds are associated with reduced hunger and altered satiety cues Tirzepatide’s dual mechanism may influence a broader range of metabolic signals in some study populations Use Across Treatment Timelines Semaglutide is frequently examined as an initial GLP-1–based option Tirzepatide is often studied later in treatment pathways or in comparative trials Individual Variability Research consistently shows wide variability in individual responses to both compounds No single approach is universally effective Interpreting Research in a Personal Context Selecting between different incretin-based therapies is not simply a matter of choosing the “newest” or “strongest” option. Research increasingly supports a personalised, adaptive approach. Key considerations often discussed in clinical literature include: 1. Starting Context For individuals new to GLP-1–based treatments, semaglutide is frequently examined as an introductory option due to its long history of study and established dosing frameworks. 2. Response Over Time Ongoing monitoring is central to research-led approaches, including observation of: Appetite regulation Tolerance and side-effect profiles Changes in metabolic markers When responses plateau or change, alternative approaches may be evaluated in controlled settings. 3. Longer-Term Objectives Short-term metabolic changes and long-term sustainability are often assessed separately in research. Some studies explore whether transitioning between therapies may better align with evolving physiological responses over time. Why Treatment Transitions Are Studied Modern metabolic research recognises that treatment strategies may change as physiology adapts. Switching between therapies does not necessarily indicate failure; instead, it may reflect refinement and optimisation. Common Research Themes Include: Plateau EffectsMetabolic adaptation over time is well documented. Dual-pathway agents are studied for their ability to engage different hormonal signals when progress slows. Tolerance and ComfortIndividual tolerability varies. Research frequently compares side-effect profiles and subjective comfort between compounds. Phase-Based ApproachesSome frameworks describe treatment in phases: Initiation and behavioural adjustment Active metabolic change Maintenance and long-term stabilisation Different compounds may be studied at different points along this continuum. The Role of Professional Oversight While educational content can provide helpful context, clinical decision-making always requires professional input. Research-guided care typically involves: Comprehensive health assessment Ongoing review of response and tolerance Adjustment or transition based on observed outcomes No medication strategy should be viewed as static or universally applicable. Final Perspective: A Flexible, Evidence-Led View Semaglutide and tirzepatide represent two important developments in incretin-based research. Rather than positioning one as categorically superior, current evidence supports viewing them as distinct tools studied for use at different points in metabolic care. Semaglutide is widely researched as a foundational GLP-1-based therapy Tirzepatide offers a dual-pathway approach that continues to be actively investigated Transitioning between therapies may reflect thoughtful, long-term strategy rather than short-term outcomes For further educational material and structured explanations of how these therapies are discussed in real-world research contexts, resources such as Trimfast.net, alongside peer-reviewed medical literature, can provide useful background reading.